What are corticosteroids?
Corticosteroids are a class of steroid hormones that includes glucocorticoids and mineralocorticoids. However, the term “corticosteroids” is generally used to refer to glucocorticoids (1). These steroids bind to glucocorticoid receptors (GR) that are present in almost every cell in the body. Glucocorticoids are cholesterol-derived steroid hormones synthesised and secreted by the adrenal gland. They are anti-inflammatory in all tissues, and control metabolism in muscle, fat, liver and bone. Glucocorticoids also affect vascular tone, and influence mood, behaviour and sleep‒wakefulness cycles via the brain and central nervous system (CNS) (2). It is the inflammatory regulation that makes these steroids the most widely prescribed treatment worldwide for neuromuscular disease such as Duchenne muscular dystrophy.
In patients with Duchenne muscular dystrophy (DMD) the lack of dystrophin being produced causes the muscles to be susceptible to damage. The body’s ability to repair this damage reduces over time as the inflammatory response to muscle damage begins to outweigh the body’s ability to repair – this results in a build up of fibrotic tissue (non-contracting tissue) replacing healthy muscle tissue which reduces strength and flexibility (1, 3). This is where the glucocorticoids come in – they are primarily used to suppress the inflammatory response and promote prolonged muscle health and strength. When glucocorticoids enter our cells they activate a chain of events (referred to as downstream events) that results in the activation of genes in response to stressors and by inhibiting pro-inflammatory regulators. One of these regulators is called Nuclear factor kappa-light-chain-enhancers of activated B cells (NF-kB). By suppressing NF-kB, inflammation is also suppressed. Glucocorticoids act to inhibit NF-kB by trapping it in an inactive state in the cells’ cytoplasm which suppresses any inflammatory response.
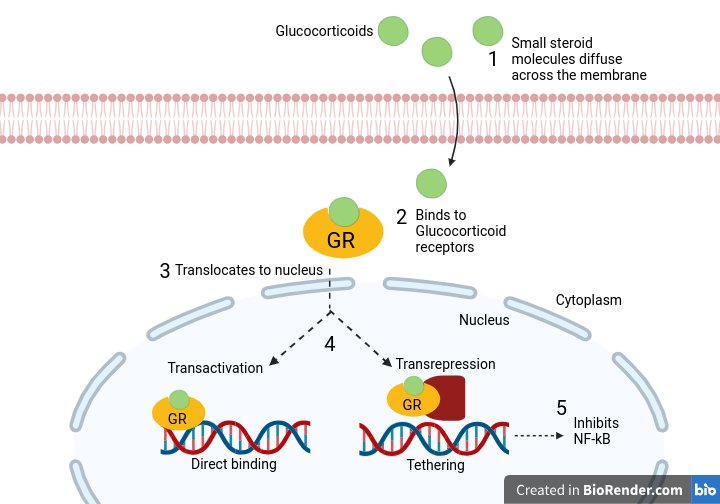
- Glucocorticoids enter the cell via diffusion
- They bind with the Glucocorticoid receptor to form a receptor-ligand complex
- The GR-ligand complex translocates to the nucleus to interact with the DNA
- Interaction is direct via transactivation (activating target genes) or indirect via transrepression
- The action of interest for steroids is the suppression of NF-kB
Side effects:
The issue with prolonged use of steroids as a treatment are the well documented side effects that lead to issues further down the line for Duchenne patients and families, such as:
- Weight gain
- Stunted growth
- Osteoporosis (weakening of bones)
- Adrenal atrophy/ suppression
- Increased infection susceptibility
- Hypertension
- Sleeping issues
- Behavioural/ emotional dysregulation
- Glucose intolerance
- Gastrointestinal irritation
- Cushingoid appearance
Weight gain, stunted growth, osteoporosis and adrenal atrophy are among the most common side effects, but all have been reported with long term use of steroids in Duchenne patients. Despite the side effects of steroid use, the alternative is an accelerated muscle degeneration and increased fibrosis (both skeletal and smooth muscle). So, the decision to take daily steroid treatments is often encouraged, and the side effects are monitored regularly and mitigated wherever possible by the appropriate medical professionals.
Still, there remains a need to find a steroid ‘alternative’ that will enable treatment for children of the Duchenne community with fewer side effects – helping ease the burden of this illness by improving the standard of treatment available.
What is Vamorolone?
Referred to as either Agamee (its initial discovery name) or vamorolone, this novel glucocorticoid is considered a next generation of steroid that look to minimise the side effects (particularly bone weakening) while maintaining the positive benefits, and is referred to as a ‘dissociative steroid’. Although not a steroid alternative, vamorolone has been synthesised to act differently to typical steroids, namely – reduced action as a binding agent (ligand) meaning less transactivation (associated with side effects), maintaining transrepression (reducing inflammation), and promoting membrane repair.
The below image shows the difference between the mechanism of action between the current glucocorticoids (Prednisolone in this case) and the vamorolone:
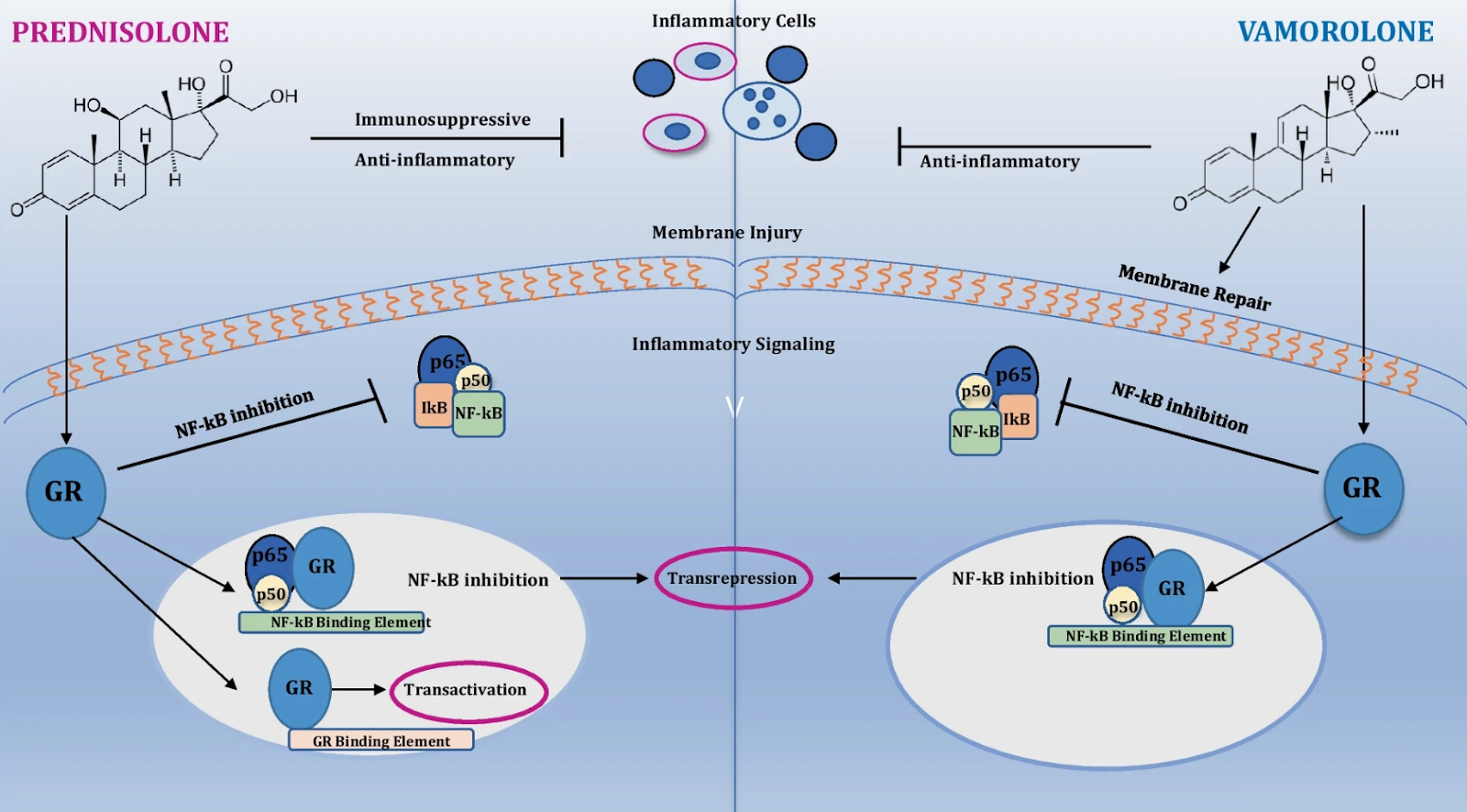
(Diagram courtesy of https://link.springer.com/article/10.1007/s13311-023-01423-y/figures/1)
Because vamorolone lacks some of the features of traditional glucocorticoids, such as increased transactivation, it specifically targets the suppression of NF-kB and inflammation. It is the transactivational pathway that is believed to be responsible for some of the adverse side effects witnessed in typical steroids (4). This lack of downstream activation is what gives rise to the term dissociative steroid.
Addressing Bone, Kidney and Brain/CNS side effects:
There are two modulator enzymes (11β-hydroxysteroid dehydrogenase 1 and 11β-hydroxysteroid dehydrogenase 2) that control the ratios of glucocorticoids in our system by binding to these steroids and either activating (referred to as ‘drug’ state) or inactivating them (referred to a ‘pro-drug’ state). These enzymes are specifically looking for a chemical signature on the steroid called a 11-β oxygen moiety to either turn it active or inactive (as indicated by the red circles in the above diagram). It is through this pathway that it is believed the most adverse side effects (particularly osteoporosis) are produced. Vamorolone has been synthesised to not contain this 11-β oxygen moiety and thus cannot be regulated by these policing enzymes and their downstream effects.
Addressing Cardiac related side effects:
Mineralocorticoids (that other class of corticosteroids) act to regulate the water and salt balance in the body. Vamorolone has been demonstrated to inhibit these mineralocorticoid receptors and there is some suggestion that this could help maintain a healthy heart as demonstrated in preclinical trials (5).
Because vamorolone is lipophilic (lipid-loving) it likes to bind to phospholipids (the material membranes are made from). Preclinical studies have demonstrated that there are some restorative functions of vamorolone that counters the lack of dystrophin that causes cell membranes to become damaged with excessive muscle length changes that causes tearing.
Overall, vamorolone is a synthetically altered glucocorticoid that has had a key element of its makeup removed in order to reduce its action as a ligand and downstream activation of cellular events that lead to the negative side effects associated with traditional steroid use in Duchenne patients.
What is the current status of clinical research?
Before we delve into the clinical trial information, it is important to understand the difference between phases of research into potential treatments (detailed info on this can be found here).
- Preclinical trials – Investigate treatments in non-human animals/ cell cultures.
- Phase 1 clinical trials – Investigate the safety of a new treatment
- Phase 2 clinical trials – Investigate the effectiveness of a new treatment
- Phase 3 clinical trials – Investigate efficacy and effectiveness compared to existing treatments in large groups of patients.
- Phase 4 clinical trials – usually post approval and continue to collect data from multiple sources of the broader population on the drugs ongoing use.
Recent approvals by the regulatory bodies EMA, FDA and MHRA are based upon the positive findings from the clinical phase 2/3 trials – A total of 12 studies on the efficacy, safety and effectiveness of vamorolone, including 1 quality measures study, 3 preclinical studies and 8 clinical studies since 2016 (6). A summary of the most recent studies is provided below:
2018 phase 2a trial reported a first-in-patient study of vamorolone in 12 boys aged 4-7 and its dissociative steroidal anti-inflammatory effects as well as increased plasma membrane stability in a 4 week long study.
2019 phase 2 trial reported a dose-related improvement in muscle function in 48 boys aged 4-7 over a 24 week period.
- Bone markers showed an increase in bone formation indicating a possible loss of this bone weakening side effect.
- insulin resistance and adrenal suppression were lower in vamorolone treated patients relative to other glucocorticoid findings.
- Higher doses of vamorolone were associated with increased physical performance including tests such as 6-minute walk test, North Star Ambulatory Assessment.
- Increased dosage was associated with a higher BMI, an indicator of unwanted weight gain.
2020 phase 2 trial, and 2022 phase 2 trial, reported the same positive benefits as other corticosteroids of anti-inflammation and improved physical assessment outcomes over an extended 18 month and 30 month period, respectively.
- Where the corticosteroids produced a stunting in growth, this side effect was observed to be significantly lower in the vamorolone treated patients.
- Contrary to the previous study, physicians treating the patients with vamorolone reported reduced weight gain, cushingoid appearance and behavioural changes compared to conventional corticosteroids (albeit these are qualitative not quantitative reports).
2022 phase 3 trial compared vamorolone to Prednisone and a placebo in a randomised, double-blind trial of 121 DMD patients aged between 4 and 7 over a 24-week treatment period between 2018 and 2021.
- Improvements were demonstrated in physical assessments including Time To Stand, 6MWT, NSAA etc in patients treated with vamorolone compared to placebo.
- Bone turnover markers declined with Prednisone but not with vamorolone.
- Yet, all 3 treatment groups led to increased adrenal insufficiency.
In all the above clinical trials, safety of this new dissociative steroid was demonstrated throughout. Although not all side effects are alleviated using vamorolone, there appear to be significantly fewer side effects demonstrated in these studies which has led to the Duchenne community calling for this new treatment to be authorised for wider use.
Current Regulatory Standings
Recently, the Medicines and Healthcare products Regulatory Agency (MHRA) followed the decision of the European Medicines Agency (EMA) by recognising the benefits of vamorolone in patients aged 4 and older. This follows the relative success of the phase 2/3 clinical trials in which there was a demonstrated an improved safety profile that has yet to be achieved by other corticosteroids.
Vamorolone has been approved with the Promising Innovative Medicine (PIM) status from the UK MHRA for DMD. However, approval is still pending by NICE for broad availability on the NHS with a decision expected on the 22nd May 2024 (7).
Vamorolone has received Fast Track and Rare Pediatric Disease designations by the U.S. FDA and granted approval as of October 2023 for patients aged 2 and older. Catalyst secured exclusive rights to sell vamorolone and will be the US-licence holder for vamorolone with plans for a commercial launch in Q1 of 2024 (8).
The difference in the time frame for acceptance by regulatory bodies between the EU, UK and US can be frustrating – leaving many to think “if one regulatory body has authorised it, why not the others?”. The answer to this valid question is rather complex, but ultimately boils down to the differences in the relationship between pharmaceutical companies, national regulatory bodies and the national health providers (in the case of the UK and EU). Thus, where public finances are being spent, there is greater emphasis on caution around efficacy and cost effectiveness. It is a difficult balance between speed to provide new treatments for communities and caution around side effects and long term use implications and sustainably supplying the treatment to those who need it in the long term.
Summary
Vamorolone is a novel corticosteroid that has so far displayed a favourable side effect profile, and in doing so has met the ever growing need for a new generation of steroid treatments for DMD patients. The hope for a new steroid treatment that can offer the benefits of reduced inflammation and preserved muscle health while reducing the impacts of side effects such as weakened bones (osteoporosis) makes this drug an exciting breakthrough in the field of neuromuscular treatments. Although studies are ongoing and the real long term effects of vamorolone will only become evident in the coming years, the benefits certainly appear to make it a more favourable option than current steroid treatments.
The US will be the first to commercialise this treatment as of Q1 in 2024, with the EU and UK set to follow suit – yet the cost effectiveness of the drug is under consideration by NICE in the UK, and its availability through the NHS is still under review.
Glossary of terms
| Corticosteroids | A steroid hormone |
| Glucocorticoid | A cholesterol derived steroid hormone |
| Mineralocorticoids | A mineral-level controlled steroid hormone |
| Enzymes | A protein that speeds up metabolism and other chemical reactions |
| Nucleus | The part of a cell that houses the DNA material |
| Phospholipid membrane | The barrier around a cell that controls what crosses into and out of the cell. |
| Cytoplasm | The controlled environment and inside space of a cell |
| Translocation | The conditional movement of proteins to the nucleus |
| Moiety | One of two approximately equal parts |
| Transactivation | The increased rate of gene expression triggered by external stimuli |
| Transrepression | The repression by GRs of gene transcription activated by other transcription factors |
| GRs | Glucocorticoid receptors – The protein complex that the glucocorticoids bind to. |
| Receptor-Ligand complex | The chemical binding of a substrate (the steroid) and the receptor (the GR). |
Useful resources on this topic:
The function and side effects of corticosteroids
The Role and function of Vamorolone
References:
- 2016, “Corticosteroids-Mechanisms of Action in Health and Disease”, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4662771/
- 2018, “Glucocorticoids: restoring balance during stress”, The Endocrinologist, https://www.endocrinology.org/endocrinologist/130-winter18/features/glucocorticoids-restoring-balance-during-stress/#:~:text=Glucocorticoids%20are%20cholesterol%2Dderived%20steroid,behaviour%20and%20sleep%E2%80%92wakefulness%20cycles.
- 2023, “Therapeutic developments for Duchenne Muscular Dystrophy”, Nature, https://www.nature.com/articles/s41582-019-0203-3
- 2023, “Evolving Therapeutic Options for the Treatment of Duchenne Muscular Dystrophy”, Neurotherapeutics, https://link.springer.com/article/10.1007/s13311-023-01423-y/figures/1
- 2019, Vamorolone targets dual nuclear receptors to treat inflammation and dystrophic cardiomyopathy, Life Science Alliance, https://europepmc.org/article/med/30745312
- 2023, “Decision Document on Paediatric Investigation Plan (PIP): Vamorolone”, MHRA, https://cms.mhra.gov.uk/pip/mhra-100811-pip01-22
- 2023, “Vamorolone for treating Duchenne muscular dystrophy [ID4024]”, NICE, https://www.nice.org.uk/guidance/indevelopment/gid-ta11135/documents
- 2023, “Santhera Marketing submission press release”, Santhera https://www.santhera.com/assets/files/press-releases/2023-03-02_MAA-MHRA-filed_e_final.pdf
 Sarepta Therapeutics Announces Positive Data from Part B of MOMENTUM, a Phase 2 Study of SRP-5051 in Patients with Duchenne Muscular Dystrophy Amenable to Skipping Exon 51
Sarepta Therapeutics Announces Positive Data from Part B of MOMENTUM, a Phase 2 Study of SRP-5051 in Patients with Duchenne Muscular Dystrophy Amenable to Skipping Exon 51